Introduction to Achilles tendon disorders:

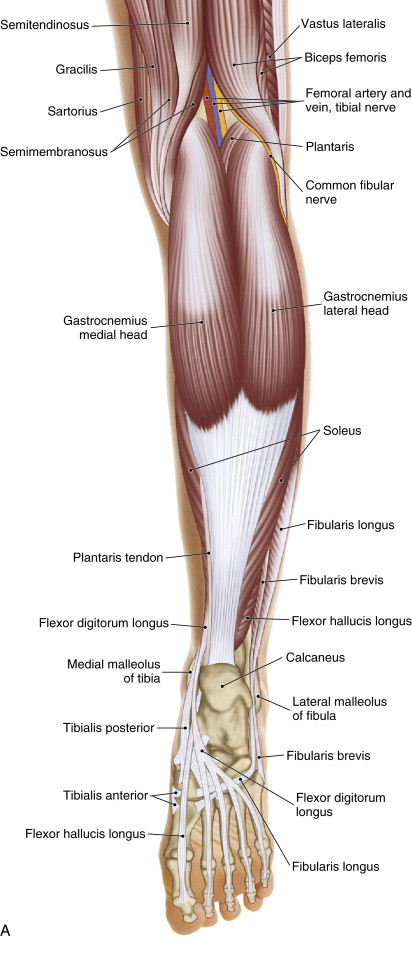
Posterior superficial view of the posterior leg/foot. Permission: Joseph E. Muscolino. The Muscle and Bone Palpation Manual, 2ed (2016), Elsevier.
The most common pathology of the Achilles tendon is Achilles tendinitis. Other disorders of the Achilles tendon are tendinosus, paratendinitis, bursitis and complete tendon rupture.
Causes:
Achilles tendinitis most often occurs due to overuse of the triceps surae group contracting to plantarflex the ankle joint. In this sense, Achilles’ tendinitis can be considered to be an overuse condition. Plantarflexing the foot at the ankle joint is important for propulsion of the support limb during the toe-off phase of the gait cycle to push the body forward when walking (and running). Therefore, excessive walking or running, or any activity or sport that involves walking or running, is most commonly the cause of Achilles’ tendinitis. This often occurs when the client/patient has had a sudden increase in the amount of activity, especially if the sedentary client/patient begins an exercise program.
Another cause of Achilles tendinitis is overstretching the ankle joint into dorsiflexion. Ankle joint dorsiflexion occurs during the gait cycle in the support limb just before toe-off. Therefore, excessive walking and/or running can also precipitate Achilles’ tendinitis due to overstretching of the tendon. Especially problematic can be eccentric contraction of the triceps surae group under load, such as when lowering into a crouch/squat position while holding a heavy weight. This requires simultaneous contraction of the triceps surae as it is stretched into dorsiflexion.
Overstretching is especially likely to occur if the triceps surae / Achilles tendon complex is tight/taut. This can occur due to chronic use of high-heel shoes. Another factor is sleeping on one’s back with the sheets tightly tucked under the mattress; this holds the feet in a position of plantarflexion, which by adaptive shortening can then result in tight gastrocnemius and soleus. Further, as a general rule, the joints of the lower extremity are more interdependent than are the joints of the upper extremity. Therefore, if the sagittal plane range of motion of the hip or knee joints is decreased, the sagittal plane range of motion of the ankle joint tends to also decrease, resulting in increased tightness of all associated musculature, including the triceps surae group. Of particular importance to manual therapists, therapists who like to generate force when working on clients from their lower extremity in back and do so solely by pushing off (plantarflexing) at the ankle joint tendon to develop tight triceps surae musculature. Better is to bend (flex) the hip and knee joints and then also push off by extending the hip joint (utilizing the glutes and hamstrings) and extending the knee joint (utilizing the quadriceps femoris).
As we age, our tissues also tend to become less elastic/plastic, increasing the chance that stretching will irritate and inflame the Achilles tendon. Both contraction and stretch of the Achilles tendon will be more problematic if the client/patient is not adequately warmed up before activity, and/or the triceps surae group is overly fatigued. Being overweight further predisposes the client/patient toward developing Achilles’ tendinitis because it increases the stress load on the Achilles tendon, requiring a stronger contraction to push off and move more weight. And previous injury to the triceps surae / Achilles tendon complex usually results in increased baseline tone and fascial adhesions, which then predisposes them to further strain injury. Further, there is some evidence that chronic use of steroidal and NSAID medication can predispose the client/patient toward disorders of the Achilles tendon due to their deleterious effect on myofascial tissue.
